4 Types of PCOS (a Flowchart)
Published from Lara Briden.com
To treat PCOS, you need to know what’s driving it. In other words, you need to know the different types of PCOS.
You could have insulin-resistant PCOS, post-pill PCOS (which is temporary), inflammatory PCOS, or the far less common adrenal PCOS.
First things first, what is PCOS?
Despite the name, polycystic ovary syndrome has nothing to do with cysts on the ovaries. The things your doctor saw on ultrasound are follicles or eggs, which are normal for the ovary. You can have many eggs and still have normal hormones, and that’s why ultrasound cannot diagnose (or rule out) the hormonal condition PCOS.
PCOS is best defined as androgen excess (high male hormones) when all other causes of androgen excess have been ruled out.
So, step 1 in determining your PCOS type is to ask “Is it really PCOS?”.
Is it really PCOS?

It’s really PCOS if you have some sign of androgen excess, such as:
- high androgens (male hormones) measurable on a blood test,
- facial hair or jawline acne.
PLUS other reasons for androgen excess have been ruled out.
Other reasons for androgen excess include certain types of birth control, congenital adrenal hyperplasia (which accounts for up to 9 percent of cases of androgen excess), and high prolactin.
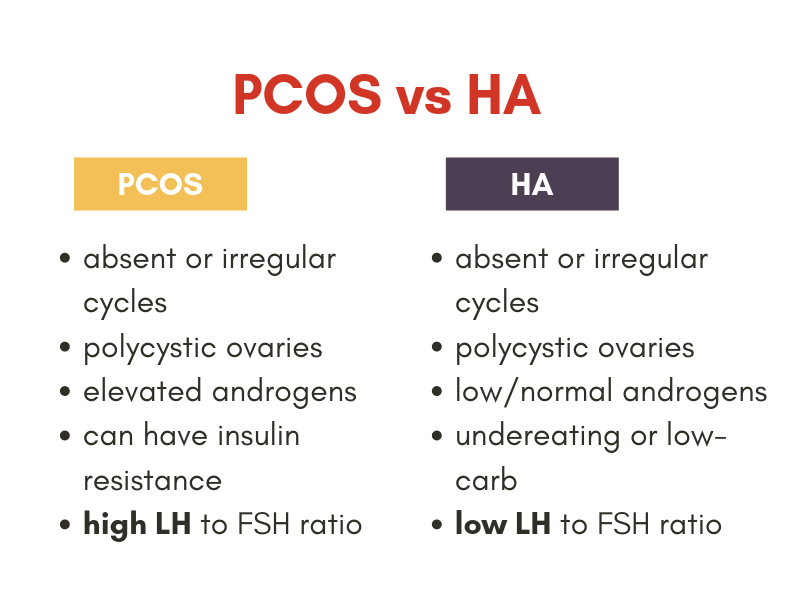
Having irregular periods (or no periods) could mean you have PCOS, or it could mean you have hypothalamic amenorrhea, which is lack of periods due to undereating or undereating carbs.
The thing to understand is that you can have polycystic ovaries with hypothalamic amenorrhea or undereating. That means you could have been mistakenly told that you have “lean PCOS” when you actually have hypothalamic amenorrhea.
For more information read:
- Maybe it’s not PCOS (and PCOS cannot be diagnosed by ultrasound)
- Pain is not a symptom of PCOS
- Is it PCOS or hypothalamic amenorrhea or both?
If you’re certain you have PCOS, then let’s move on. Do you have insulin resistance?
Insulin-resistant PCOS

Insulin resistance means having high insulin. It’s also called metabolic syndrome or pre-diabetes. The best way to test for insulin resistance is to measure the hormone insulin (not glucose).
If your insulin is high, then the high insulin is driving your androgens and you have insulin resistance and insulin-resistant PCOS.
The treatment of insulin-resistant PCOS is to reverse insulin resistance with diet, exercise, and supplements like magnesium and inositol.
Do you have insulin resistance? If you’re thinking “no,” then my next question is “are you sure?”
There’s a 70 percent chance your PCOS is insulin-resistant PCOS.
Did your doctor test for insulin or only glucose or HbA1c? Those tests are not tests for insulin resistance. For more information on insulin testing, see Chapter 7 in Period Repair Manual or my insulin blog post.
If you’re certain you do not have insulin resistance, then let’s move on. Did your symptoms start when coming off the pill?
Post-pill PCOS

It’s pretty common to experience a temporary surge in androgens when coming off a drospirenone or cyproterone pill like Yasmin, Yaz, Diane, or Brenda.
Under current diagnostic guidelines, that temporary surge in androgens is enough to qualify for the diagnosis of PCOS or post-pill PCOS.
With my post-pill PCOS patients, I recommend the following:
- Stay calm and know the symptoms are part of a temporary drug-withdrawal process.
- Consider using a natural anti-androgen supplement like zinc, DIM, or peony & licorice combination for a few months. Read the 7 best natural anti-androgen supplements.
You have post-pill PCOS if you meet the criteria for PCOS (excess androgen and other conditions ruled out), plus you do not have insulin resistance, plus symptoms started when trying to come off the pill.
If you did not just come off the pill or if you had a problem before birth control, then let’s move on. Do you have signs of chronic inflammation?
Inflammatory PCOS

Chronic inflammation can stimulate the ovaries to make too much testosterone and is a contributing factor for every type of PCOS.
When chronic inflammation is the primary factor or driver, it’s inflammatory PCOS.
The treatment for inflammatory PCOS is to identify and correct the underlying source of inflammation. That could mean avoiding a food sensitivity such as dairy, or fixing an underlying gut problem or addressing chronic mast cell activation or histamine intolerance. The supplements zinc and N-acetyl cysteine work particularly well for this type of PCOS.
You have inflammatory PCOS if you meet the criteria for PCOS, plus you do not have insulin resistance, plus you’re not in a temporary post-pill phase, plus you have signs and symptoms of inflammation, as follows:
- unexplained fatigue
- bowel problems like IBS or SIBO
- headaches
- joint pain
- a chronic skin condition like psoriasis, eczema, or hives.
If you do not have signs of chronic inflammation, then let’s move on. Do you have adrenal PCOS?
Adrenal PCOS

Most women with PCOS have an elevation of all androgens including testosterone and androstenedione from the ovaries and DHEAS from the adrenal glands.
If you have only elevated DHEAS (but normal testosterone and androstenedione), then you may have adrenal PCOS, which accounts for about 10 percent of PCOS diagnoses.
Adrenal PCOS is not driven by insulin resistance or inflammation. Instead, it’s an abnormal response to stress. Treatments include stress reduction, magnesium, adaptogen herbs (including licorice), and vitamin B5, the “anti-stress factor.”
In addition to treating the underlying driver of your PCOS, you may also require a natural anti-androgen supplement.
For information about the 4 types of PCOS and their treatments, see Chapter 7 of Period Repair Manual.
👉 Tip: Thinking you have more than one type? The types are listed in order of priority. So, if you have insulin resistance, then you have insulin-resistant PCOS — even if you also have inflammation and a post-pill situation.
Still confused?
What if you’ve been told you have PCOS, but you do not seem to meet any of the criteria discussed here?
Go back to the drawing board. Do you truly have PCOS? As in, do you have high androgens? Either measurable on a blood test or the clear physical sign of facial hair.
👉 Tip: Your androgen symptoms could be from birth control. Some progestins such as levonorgestrel are very “testosterone-like” and cause acne and hair loss. Read 4 causes of androgen excess in women.
Because if you don’t have high androgens, and lack of periods (and maybe mild acne) is your only symptom, then you could actually have hypothalamic amenorrhea. (And look at your luteinizing hormone — it’s high with PCOS and low with hypothalamic amenorrhea.)
{kind=link}
Recent Comments